Biomed. adv. 1(1):42-45.
doi: 10.34172/bma.07
Case Report
A rare case of double chamber left ventricle misdiagnosed as a pseudo-aneurism in cardiac magnetic resonance imaging: Case report
Rezvaniyeh Salehi Conceptualization, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing, 1, * 
Rezayat Parvizi Conceptualization, 1
Ramin Foroughi Asl Data curation, 1
Kasra Mirzazadeh Investigation, 2
Mahsa Zehisaadat Data curation, Investigation, Writing – original draft, Writing – review & editing, 1
Author information:
1Cardiovascular Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
2Faculty of Medicine, Medical University of Gdansk, Gdansk, Poland
Abstract
Summary
A double chambered left ventricle (DCLV) is an extremely rare congenital malformation. In this anomaly left ventricle (LV) is divided into two sub-sections by a muscle bundle or a septum: main left ventricular chamber (MLVC) and accessory chamber. The reported prevalence of DCLV is 0.04%-0.42%; however, the precise prevalence is not determined. In this case, we are reporting a 54 years old man who was referred to cardiologist with a complaint of chest pain. He had a history of systemic hypertension. With regard to echocardiographic findings, the patient was diagnosed to have a left ventricular aneurism or DCLV. For further evaluation, cardiac magnetic resonance imaging (CMRI) was recommended. The results of CMRI revealed pseudo-aneurism with laminated thrombus. Nonetheless, through cardiac surgery DCLV with thick bundles was diagnosed. DCLV is rarely detected in adult patients since, in case of presence, it is mainly diagnosed during infancy or early childhood. Echocardiography is the initial imaging tool for diagnosis of DCLV; however, CMRI improves the chance of accurate diagnosis of the condition by providing a more detailed view.
Keywords: Double chamber left ventricle, Congenital heart disease, Echocardiography, Cardiac magnetic resonance imaging, Pseudo-aneurism
Copyright and License Information
© 2024 The Author(s).
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Introduction
Outpouching of left ventricle (LV) is a rare condition with variable etiologies including congenital heart problems, complications of coronary artery disease and myocardial infarction (aneurisms and pseudo-aneurysms), LV false tendon, LV fibrosis and diverticula. Considering that determining the etiology is clinically challenging, imaging evaluations play a fundamental role in management of these cases. LV outpouching or subdivision is rare in comparison to right ventricle. The divided chambers are usually separated by muscle bands or anomalous septum.
Nowadays, new imaging modalities such as echocardiography, contrast enhanced echocardiography, 3-dimensional echocardiography and cardiac magnetic resonance imaging (CMRI) are useful in thorough assessment of structural complications. Through CMRI, it is also possible to observe ventricular contractility, inflammation and fibrosis.1-5
Pathogenesis in congenital forms of double chambered left ventricle (DCLV) may be associated with hypoplasia of regional myocardial intra-trabecular sinusoid, intra myocardial aneurysm formation during myocardial embryogenesis,6 incomplete ventricular trabecular regression or a variant of non-compaction LV. 7
Like other myocardial abnormalities such as hypertrophic or dilated cardiomyopathies, genetic causes may be involved.8
Other poorly defined terms exist as well in available literature including LV diverticulum, LV aneurysm, LV cysts and accessory LV chamber.9 The most important differential diagnoses of DCLV are LV diverticulum and LV aneurysm. LV diverticulum is distinguished from DCLV by its morphology; as it has a narrow neck connecting to LV cavity. During echocardiography, presence of subdivision of LV to two distinct contracting chambers could be a sign of DCLV; though, the accessory chamber has not necessarily contractile function in all the patients with DCLV.5
LV true aneurysm is a saccular protrusion of LV wall with a wide neck and scarred /fibrotic tissue happening due to mechanical weakness and contains all three cardiac layers. Aneurysms appear in echocardiography as an akinetic or dyskinetic segment in LV.10 LV pseudo-aneurysm does not contain all the three layers of myocardium and has a high probability of rupture. Echocardiographic appearance of a pseudo-aneurysm is a dyskinetic segment.2
Herewith, we describe a case of DCLV, with an emphasis on the importance of imaging in addition to echocardiography.
Case Presentation
A 54 years old man was referred to cardiologist with a complaint of recent non-anginal chest pain and palpitation. His past medical history revealed stage 1 systemic hypertension which was controlled by a daily dose of 25 mg losartan and a hospital admission due to anteroseptal myocardial infarction. Findings of physical examination were as: blood pressure = 110/80 mm Hg, heart rate = 75 bpm, muffled S1, normal P2 and no audible cardiac murmur. His electrocardiograph revealed incomplete left bundle branch block.
Echocardiographic evaluation unveiled normal LV size with global ejection fraction of 40% and large apical outpouching in size of 53 mm and a 25 mm neck. Color flow Doppler mode revealed bidirectional flow and mildly dilated ascending aorta. (Figures 1-3 demonstrate the Echocardiography views obtained from the patient.)
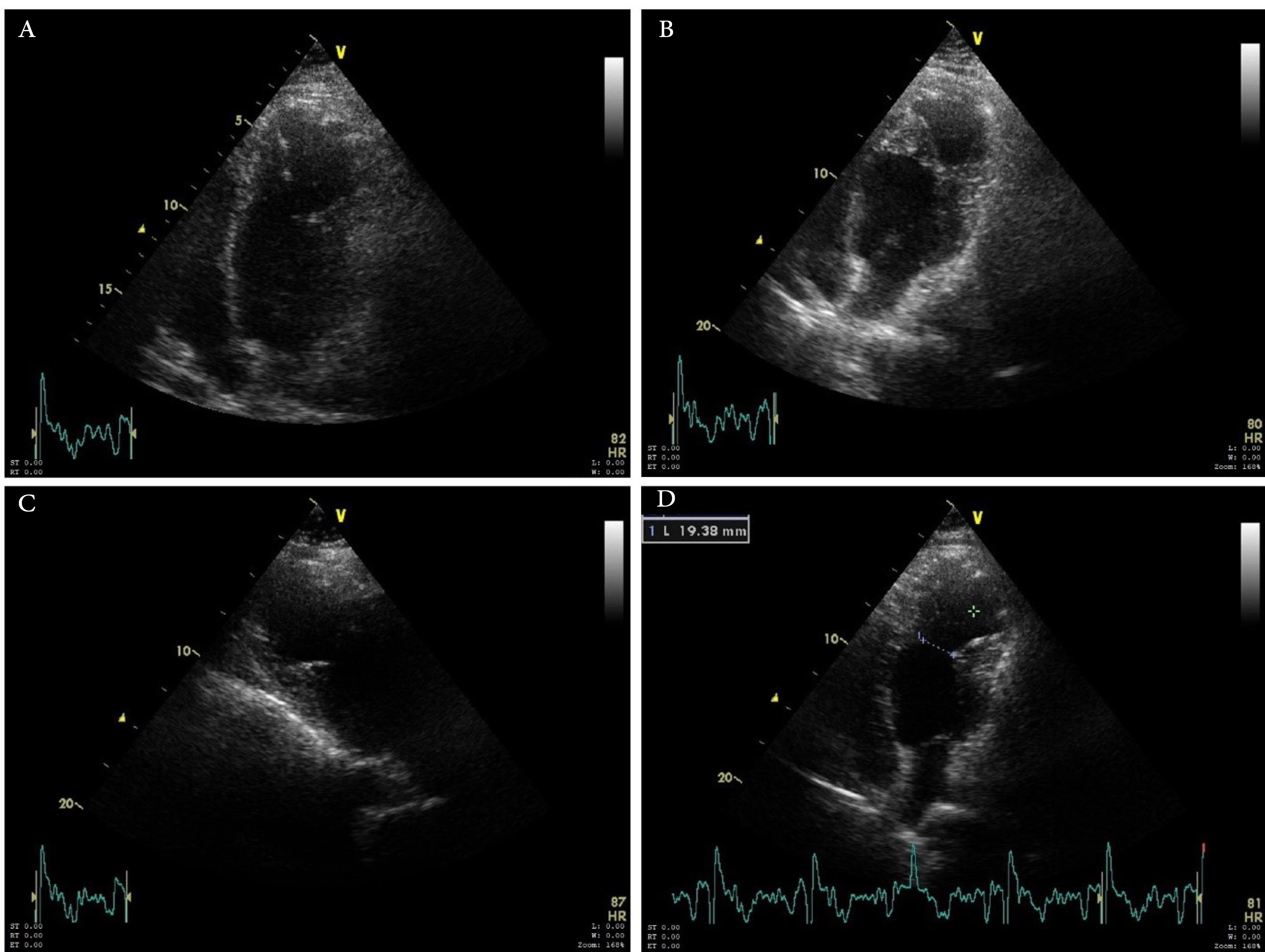
Figure 1.
Apical chamber views. A, B, D represented an apical four chamber views and figure C revealed apical long axis view.
.
Apical chamber views. A, B, D represented an apical four chamber views and figure C revealed apical long axis view.
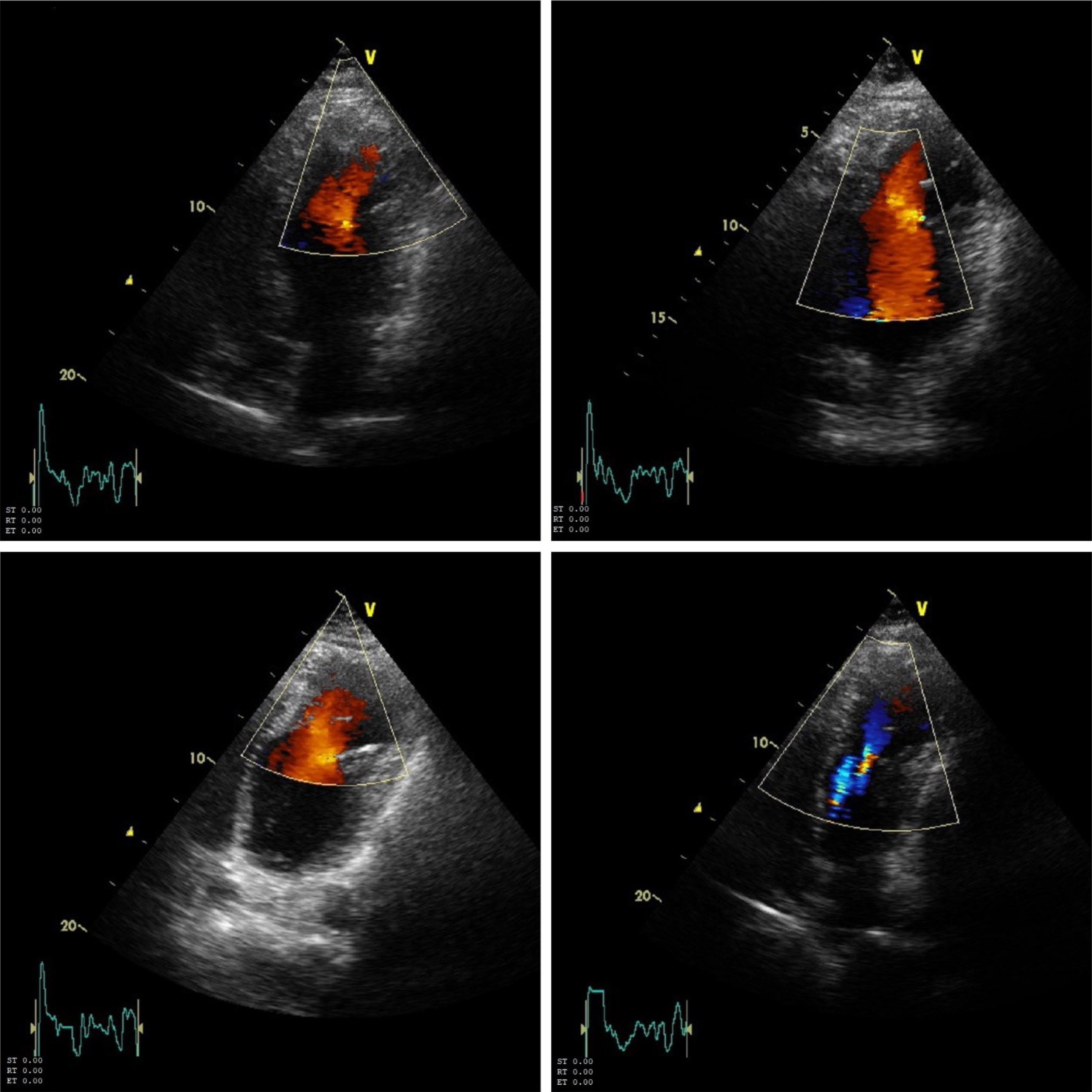
Figure 2.
Color doppler flow imaging of left ventricular of the same patient.
.
Color doppler flow imaging of left ventricular of the same patient.
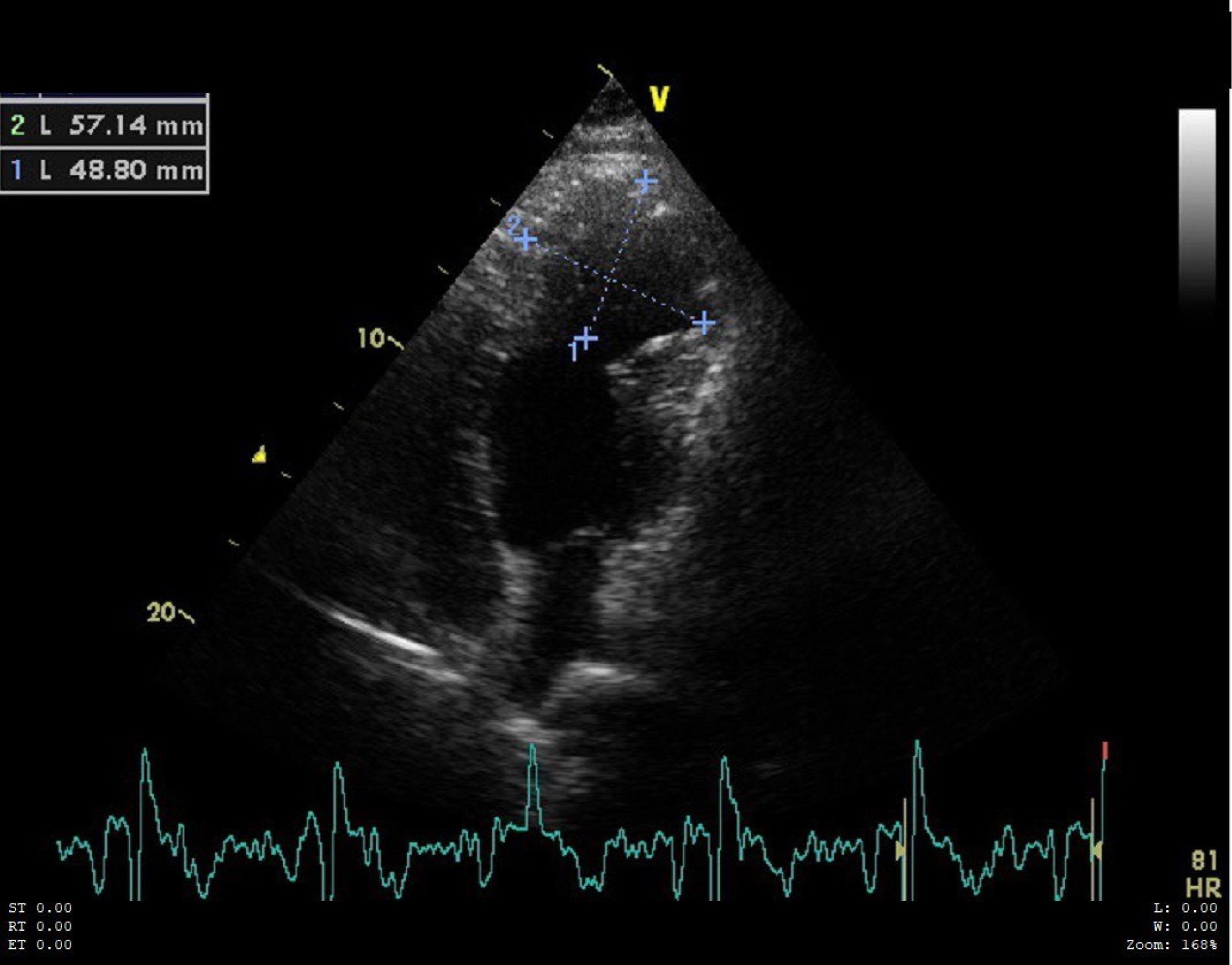
Figure 3.
Left ventricular apical aneurysm size in four chamber views.
.
Left ventricular apical aneurysm size in four chamber views.
Echocardiologist recommended CMRI regarding that the accessory chamber was free of clot and had occasional contractions. CMRI was performed with 1.5 tesla, 18 canal Avanto Siemens scanner. In the results, LV apical pseudo-aneurysm with laminated thrombus was reported. In coronary angiography a non-significant lesion in distal part left ascending artery was present.
Concerning the diagnosis of apical pseudo-aneurysm, the patient underwent surgery and through the operation thick fibrotic mid LV ring with aneurysmal apex were found.
Patient post-operative course was uneventful and follow up echocardiography showed an ejection fraction of 40%.
Discussion
DCLV is characterized by the sub-division of the LV chamber into two chambers by abnormal muscular tissue. It is differentiated from LV aneurysm and pseudo-aneurysm by visualization of contractile function during systole in both chamber and also slight expansion due to increased pressure during systole.11,12
In contrast to double chamber right ventricle, which is associated with septal defect, tetralogy of Fallot and/or transposition of great arteries, DCLV is commonly silent. In DCLV, there is a low pressure gradient between two chambers because of parallel position of main and accessory chambers. From etiologic point of view, DCLV is less known; but it is thought to be congenital and non-progressive.13,14
CMRI with normal delayed enhancement images is suggestive for ruling out coronary artery diseases and fibrosis.
Usually, DCLV is an incidental finding in the course of cardiovascular imaging. It is a rare condition with no definite available data regarding the outcome, prognosis and risk of embolism; nevertheless, it is generally believed that thromboembolic risk is low and treatment is guided by the presence of associated abnormalities.3,15,16
We believe that the misdiagnosis of DCLV during CMRI was probably due to a poor thoracic window that did not provide proper diagnostic-quality images of this condition.
Conclusion
Double Chamber Left Ventricle is a rare cardiac malformation which is characterized by LV sub-division to main and accessory LV cavities. Usually being diagnosed during neonatal or pediatric age, it rarely remains asymptomatic until adulthood as in our case. Echocardiography can aid the detection of DCLV; however, CMRI allows a better evaluation and tissue characterization. In our case the coarse bundles inside the accessory chamber were confused with laying thrombosis in CMRI. With respect to the rarity of this anomaly, there are few evidence-based treatment approaches and the prognosis is poorly determined.
Competing Interests
The authors declare no potential conflict o9f interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent was obtained from the participant for anonymized patient information to be published in this article.
References
- Nacif MS, Mello RA, Lacerda Junior OO, Sibley CT, Machado RA, Marchiori E. Double-chambered left ventricle in an adult: diagnosis by CMRI. Clinics (Sao Paulo) 2010; 65(12):1393-5. doi: 10.1590/s1807-59322010001200028 [Crossref] [ Google Scholar]
- Akdemir R, Balci MM, Ozer C, Karcaaltincaba M, Acikel S. Quadrichambered ventricles. Cardiol J 2010; 17(3):303-5. [ Google Scholar]
- Köz C, Yokuşoğlu M, Uzun M, Baysan O, Bulakbaşi N. Double-chambered left ventricle with nonsustained ventricular tachycardia. Anadolu Kardiyol Derg 2009; 9(3):E5. [ Google Scholar]
- Breithardt OA, Ropers D, Seeliger T, Schmid A, von Erffa J, Garlichs C. A heart within the heart: double-chambered left ventricle. Eur J Echocardiogr 2008; 9(5):739-41. doi: 10.1093/ejechocard/jen158 [Crossref] [ Google Scholar]
- Zhang XY, Cao TS, Yuan LJ. Double-chambered left ventricle in echocardiography. Echocardiography 2012; 29(3):E67-8. doi: 10.1111/j.1540-8175.2011.01569.x [Crossref] [ Google Scholar]
- Gufler H, Anderson RH, Annette M, Voigtlaender T. Double-chambered left ventricle in a patient with chest pain. Clin Res Cardiol 2018; 107(12):1180-2. doi: 10.1007/s00392-018-1298-z [Crossref] [ Google Scholar]
- Novo G, Dendramis G, Marrone G, Novo S, Thiene G. Left ventricular noncompaction presenting like a double-chambered left ventricle. J Cardiovasc Med (Hagerstown) 2015; 16(7):522-4. doi: 10.2459/jcm.0000000000000264 [Crossref] [ Google Scholar]
- Wang J, Zhang X, Wang X, Wang C, Wang F, Wang B. MYH7 rare variant in a family with double-chambered left ventricle. Circ Cardiovasc Genet 2017; 10(6):e001729. doi: 10.1161/circgenetics.117.001729 [Crossref] [ Google Scholar]
- Bilici M, Demir F, Akın A, Güzel A, Akdeniz O, Tan İ. Echocardiographic diagnosis of double-chambered left ventricle. J Echocardiogr 2016; 14(4):176-8. doi: 10.1007/s12574-016-0297-1 [Crossref] [ Google Scholar]
- Zoffoli G, Mangino D, Venturini A, Terrini A, Asta A, Zanchettin C. Diagnosing left ventricular aneurysm from pseudo-aneurysm: a case report and a review in literature. J Cardiothorac Surg 2009; 4:11. doi: 10.1186/1749-8090-4-11 [Crossref] [ Google Scholar]
- Awad SM, Patel AS, Polimenakos A, Braun R, Abdulla RI. Left ventricular accessory chamber: a case report and review of the literature. Pediatr Cardiol 2009; 30(7):1022-5. doi: 10.1007/s00246-009-9482-6 [Crossref] [ Google Scholar]
- Gerlis LM, Partridge JB, Fiddler GI, Williams G, Scott O. Two chambered left ventricle Three new varieties. Br Heart J 1981; 46(3):278-84. doi: 10.1136/hrt.46.3.278 [Crossref] [ Google Scholar]
- Kilner PJ, Geva T, Kaemmerer H, Trindade PT, Schwitter J, Webb GD. Recommendations for cardiovascular magnetic resonance in adults with congenital heart disease from the respective working groups of the European Society of Cardiology. Eur Heart J 2010; 31(7):794-805. doi: 10.1093/eurheartj/ehp586 [Crossref] [ Google Scholar]
- Choi YJ, Park SW. Characteristics of double-chambered right ventricle in adult patients. Korean J Intern Med 2010; 25(2):147-53. doi: 10.3904/kjim.2010.25.2.147 [Crossref] [ Google Scholar]
- Kay PH, Rigby M, Mulholland HC. Congenital double chambered left ventricle treated by exclusion of accessory chamber. Br Heart J 1983; 49(2):195-8. doi: 10.1136/hrt.49.2.195 [Crossref] [ Google Scholar]
- Partington SL, Ali B, Daly RP, Koplan BA, Lilly LS, Solomon SD. Images in cardiovascular medicine Initial presentation of an accessory left ventricle in a patient with syncope. Circulation 2010; 121(19):e401-3. doi: 10.1161/CIR.0b013e3181e036bf [Crossref] [ Google Scholar]